Septoplasty: Correcting a Deviated Septum to Improve Nasal Breathing
- 6 days ago
- 6 min read
Written by Mr Tim Biggs | Consultant ENT Surgeon | Rhinology & Facial Plastics
What Is the Nasal Septum?
The nasal septum is the internal partition that divides the nose into left and right sides. It is composed of cartilage at the front and thin bone at the back, covered on both surfaces by a layer of mucosa. In an ideal world, the septum sits centrally, dividing the nasal airway into two roughly equal passages. In practice, a perfectly central septum is the exception rather than the rule.
Minor degrees of septal deviation are extremely common and in most people cause no meaningful symptoms. Problems arise when the deviation is more significant, narrowing one or both nasal passages to the point where airflow is restricted and the patient notices a persistent blocked nose, one-sided or alternating obstruction, difficulty sleeping, or impaired exercise tolerance.
What Causes a Deviated Septum?
Septal deviation has two main origins. The first is developmental, where asymmetric growth of the septum during childhood and adolescence results in a natural curvature or angulation. Many people are unaware they have a deviated septum until it is identified during a clinical examination for another reason.
The second cause is trauma. A blow to the nose, whether from sport, an accident, or a physical altercation, can displace or fracture the septal cartilage, resulting in acute or gradually worsening deviation. Patients who experienced a nasal injury in their youth sometimes notice increasing obstruction years later as the initially minor displacement becomes more pronounced with age.
Symptoms of a Deviated Septum
The cardinal symptom is nasal obstruction. This may affect one side predominantly, or patients may describe an alternating blockage that shifts between sides depending on position or time of day. Other symptoms that commonly accompany significant septal deviation include:
• Mouth breathing, particularly at night
• Snoring and disturbed sleep
• Recurrent nosebleeds, caused by turbulent airflow drying the nasal mucosa at the point of deviation
• Recurrent sinusitis, where the deviation obstructs sinus drainage pathways
• Reduced exercise tolerance due to impaired nasal airflow
• Headache or facial pressure, in cases where the deviated septum contacts the lateral nasal wall
It is worth noting that a deviated septum rarely acts in isolation. Concurrent turbinate hypertrophy, where the nasal lining tissue on the wider side of the nose enlarges to compensate for the additional space, is extremely common and often contributes as much to obstruction as the deviation itself. Addressing both at the same time is important for achieving a good functional result.
Diagnosis: What to Expect at Consultation
Diagnosis is straightforward and is made by nasal endoscopy. Using a fine rigid endoscope passed through the nostril, I can directly visualise the septum, identify the nature and extent of any deviation, and assess the turbinates and the rest of the nasal cavity. This takes only a few minutes, requires no preparation, and is well tolerated.
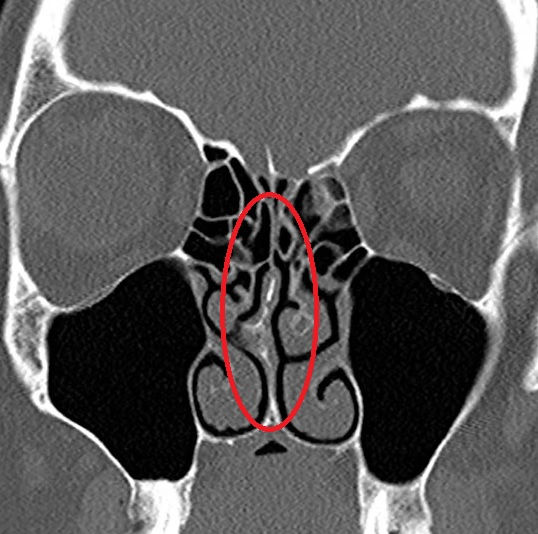
In most straightforward cases, no further investigation is needed before proceeding to surgery. A CT scan of the sinuses may be requested if there is accompanying sinus disease, or where the anatomy is complex and surgical planning requires more detail.
What Is Septoplasty?
Septoplasty is the surgical procedure to straighten and reposition a deviated nasal septum. It is performed entirely through the nostrils, with no external incisions and no visible scarring. General anaesthetic is used, and it is almost always performed as a day-case procedure.
Through a small internal incision, I elevate the mucosal lining from the underlying cartilage and bone, reposition or remove the deviated portions, and replace the mucosa. The goal is to straighten the central partition sufficiently to restore a functional airway on both sides, while preserving as much cartilage as possible for structural support. Where significant cartilage deviation cannot be corrected by repositioning alone, a technique called extracorporeal septoplasty, where the cartilage is removed, reshaped on a board, and reimplanted, may be used for more complex cases.
I do not use nasal packing after septoplasty. Patients breathe through the nose immediately after surgery and consistently report a more comfortable recovery as a result.
Combining Septoplasty With Turbinate Reduction
As noted above, turbinate hypertrophy on the wider side of a deviated nose is almost universal. Correcting the septum without addressing enlarged turbinates frequently leaves patients disappointed with the functional result, because the turbinate now occupies the space that the septum has vacated.
Where indicated, I combine septoplasty with submucosal turbinate reduction using a microdebrider, which precisely reduces the bony and soft tissue bulk of the turbinate while preserving the mucosal surface. This combined procedure is highly effective and does not add significantly to recovery time. For patients seeking both functional and cosmetic improvement, septoplasty can also be incorporated into a full septorhinoplasty.
Recovery After Septoplasty
The First Week
The nose will feel congested and blocked for the first week or two due to internal swelling. This is normal and does not mean the surgery has not worked. There may be some blood-stained discharge and mild discomfort, managed comfortably with simple analgesia. Nasal saline douching begins the day after surgery to keep the internal cavity clean and support healing.
Returning to Normal Activity
Most patients return to desk-based work and normal daily activity within one to two weeks. Strenuous exercise, contact sport, and heavy lifting are avoided for two weeks. Air travel is best deferred for two weeks. A review appointment is arranged at around six weeks to assess the functional outcome.
When Will I Notice the Improvement?
Functional improvement is gradual as internal swelling subsides. Most patients appreciate a meaningful difference by four to six weeks, with the full benefit of surgery apparent by three months. I counsel patients to be patient with this timeline, as premature assessment at two or three weeks will not reflect the final result.
Risks and Limitations
Septoplasty is a safe and well-established procedure. As with all surgery, there are risks that I discuss openly at consultation:
• Incomplete correction, where residual or recurrent deviation limits the functional outcome
• Perforation of the septum, a rare but recognised complication that is usually asymptomatic but can cause crusting or whistling
• Temporary numbness of the upper front teeth, which resolves in most cases
• Bleeding, the risk of which is minimised by technique and no-packing management
• General anaesthetic risks, which are low in healthy individuals
Septoplasty does not change the external appearance of the nose. Patients who wish to address cosmetic concerns at the same time should discuss combined septorhinoplasty at consultation.
Arrange a Consultation
If nasal obstruction is affecting your sleep, exercise, or quality of life, I would be glad to assess you. A consultation includes nasal endoscopy, a thorough review of your symptoms, and a clear discussion of whether septoplasty, a combined procedure, or a non-surgical approach is most appropriate for you.
I see patients privately at Medicana Hospital in Winchester and Adnova Clinic in Fareham. To arrange a consultation, please contact my secretary Michele Hewlett. Fees are available at www.hampshireentclinics.co.uk.

Frequently Asked Questions
What is a deviated septum?
The nasal septum is the central partition dividing the nose into left and right sides. A deviated septum is one that is displaced or bent to one side, narrowing one or both nasal passages and reducing airflow. Deviation may be congenital or caused by nasal trauma.
What is septoplasty?
Septoplasty is a surgical procedure to straighten and reposition a deviated nasal septum. It is performed entirely through the nostrils under general anaesthetic, with no external cuts or visible scarring, and is a day-case operation.
Will septoplasty change the appearance of my nose?
Septoplasty alone is a functional procedure and does not alter the external appearance of the nose. If cosmetic change is also desired, a rhinoplasty or septorhinoplasty will be needed.
How long does recovery take after septoplasty?
Most patients return to normal activity within one to two weeks. There is no nasal packing. The nose may feel congested for the first few weeks as internal swelling settles. Full functional improvement is usually appreciated by six to eight weeks.
Is nasal packing used after septoplasty?
No. Mr Biggs does not use nasal packing after septoplasty. Packing is uncomfortable and the evidence does not support its routine use. Patients report a more comfortable recovery without it.
Can a deviated septum cause snoring or sleep problems?
Yes. Significant nasal obstruction from a deviated septum can contribute to snoring and worsen obstructive sleep apnoea. Improving nasal airflow through septoplasty may reduce snoring, though it does not reliably treat established sleep apnoea in isolation.
Where does Mr Tim Biggs perform septoplasty?
Mr Biggs performs septoplasty privately in Hampshire.
How do I find out the cost of septoplasty?
Fees are listed at www.hampshireentclinics.co.uk. To book a consultation, contact Michele Hewlett, Mr Biggs's secretary.