Septoplasty and Turbinate Reduction Combined: Addressing All Causes of Nasal Obstruction
- Apr 20
- 4 min read
Written by Mr Tim Biggs | Consultant ENT Surgeon | Rhinology & Facial Plastics
Why the Septum and Turbinates Are Rarely Independent Problems
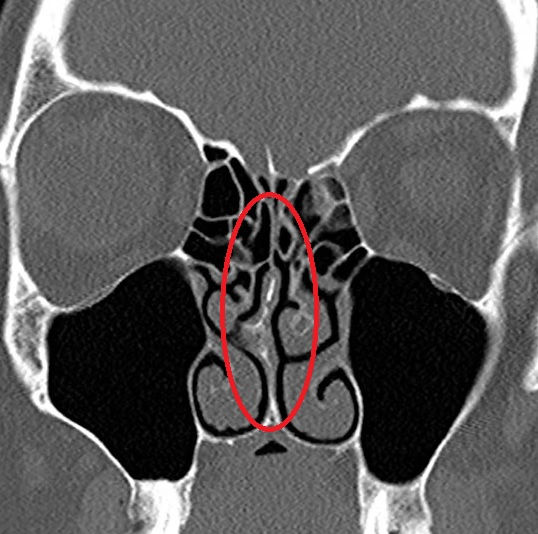
Nasal obstruction is rarely caused by just one structure acting in isolation. In most patients presenting with a significantly deviated septum, there is a co-existing abnormality of the inferior turbinates that contributes equally to obstruction. Understanding why requires a brief look at the anatomy.
When the nasal septum deviates to one side, the nasal cavity is asymmetric: narrow on the side to which the septum deviates, and wider on the opposite side. The inferior turbinate, a highly vascular structure, responds to this chronic asymmetry by enlarging on the wider side, a process known as compensatory hypertrophy. The turbinate is, in effect, partially filling the extra space created by the deviation.
The consequence is predictable: correcting the septal deviation creates a more central partition, but if the compensatorily enlarged turbinate is not addressed at the same time, it now occupies the space that the septum has vacated. The patient emerges from septoplasty with a straight septum but still feels blocked, because the turbinate problem has not been solved.
The Common Scenario: Disappointing Results After Septoplasty
Persistent obstruction after septoplasty is one of the most common reasons patients seek a second opinion in rhinology practice. It is a frustrating experience: the patient has undergone an operation under general anaesthetic, been told their septum was straightened, and yet still cannot breathe comfortably through the nose.
In many of these patients, the septoplasty has been done well and the septum is indeed straight. The problem is that the turbinate hypertrophy was not identified or addressed at the original operation. A fresh assessment with nasal endoscopy will clarify this diagnosis and determine whether turbinate reduction, performed as a standalone or revision procedure, would produce the improvement the original surgery failed to achieve.
Other causes of post-septoplasty obstruction include residual or recurrent septal deviation, adhesion formation (synechiae) between the septum and lateral nasal wall, and nasal valve collapse, where the structural support of the nasal sidewall has been compromised. Each requires a specific approach, and careful endoscopic assessment is the starting point.
Why Combining Both Procedures Makes Sense - septoplasty and turbinate reduction
For patients who have not yet had any surgery, the case for addressing both the septum and the turbinates in a single operation is compelling:
• Better functional outcome: the nasal airway is comprehensively optimised in one procedure rather than leaving a known contributor to obstruction unaddressed
• Single general anaesthetic: one admission, one recovery period, and one set of risks rather than two
• No added recovery time: the combined procedure does not significantly extend recovery compared to either operation performed alone
• Avoidance of revision surgery: patients who have both issues addressed together are far less likely to require a second operation for residual obstruction
The combination of septoplasty with submucosal microdebrider turbinoplasty is the procedure I most commonly perform for nasal obstruction. It is reliable, well-tolerated, and produces excellent long-term functional results when the correct indications are present.
What the Combined Operation Involves
The procedure is performed under general anaesthetic through the nostrils, with no external incisions and no visible scarring. I first address the septum, repositioning or removing the deviated cartilage and bone to centralise the partition. I then perform submucosal microdebrider turbinoplasty on the enlarged inferior turbinate or turbinates, removing the bony and soft tissue bulk from beneath the mucosal surface while leaving the mucosa intact.
The operation typically takes 45 to 60 minutes and is performed as a day-case procedure. There is no nasal packing. Patients breathe through the nose immediately after surgery and are discharged the same day.
Recovery
The recovery after combined septoplasty and turbinate reduction is essentially the same as for either procedure alone. The nose will feel congested for the first one to two weeks as internal swelling settles. Nasal saline douching begins from the first post-operative day. Most patients return to normal daily activity within one to two weeks, with the full functional benefit apparent by six to eight weeks.
Can This Be Combined With Rhinoplasty?
Yes. For patients who also wish to address the external appearance of the nose, septoplasty and turbinate reduction can be incorporated into a full septorhinoplasty. This is particularly relevant for patients who have breathing problems alongside cosmetic concerns, and it is one of the most common combinations I perform at Adnova Clinic, where the full range of structural and cosmetic rhinoplasty techniques is available alongside functional airway surgery.
Arrange a Consultation
Whether you are considering nasal airway surgery for the first time or seeking a second opinion following a previous operation, I would be glad to assess you. Nasal endoscopy will clarify the precise cause of your obstruction and allow us to discuss the most appropriate and effective surgical plan.
I see patients privately. To arrange a consultation, please contact my secretary Michele Hewlett. Fees are available at www.hampshireentclinics.co.uk.
Frequently Asked Questions
Why is turbinate reduction often needed alongside septoplasty?
When the septum deviates to one side, the inferior turbinate on the wider side enlarges compensatorily. Correcting the septum without addressing this turbinate leaves the patient with an enlarged turbinate occupying the corrected space, producing a disappointing functional result.
Is it safe to have both procedures at the same time?
Yes. Combining septoplasty with turbinate reduction under the same anaesthetic is standard practice. It does not significantly increase operative time, risk, or recovery, and produces a better functional outcome.
What if I already had septoplasty but am still blocked?
Persistent obstruction after septoplasty is often due to turbinate hypertrophy not addressed at the original operation, or nasal valve compromise. A specialist endoscopic assessment will identify the cause and determine the appropriate revision procedure. It could also represent nasal valve collapse.
How long does the combined operation take?
Combined septoplasty with bilateral turbinate reduction typically takes 45 to 60 minutes under general anaesthetic and is performed as a day-case procedure.
Where does Mr Tim Biggs perform this combined procedure?
Mr Biggs performs combined septoplasty and turbinate reduction privately in Hampshire.
How do I find out the cost?
Fees are listed at www.hampshireentclinics.co.uk. Contact Michele Hewlett, Mr Biggs's secretary, to arrange a consultation.


